Is that seemingly harmless manicure, or the quest for perfectly polished nails, potentially harboring a hidden health hazard? Contact dermatitis, a common yet often underestimated skin condition, is increasingly linked to the very products designed to beautify our hands and feet.
The world of nail cosmetics, with its dazzling array of gels, polishes, and acrylics, has become a multi-billion dollar industry. Yet, lurking within these alluring products are chemicals that can trigger a cascade of adverse reactions, from mild irritation to debilitating allergic responses. This article delves into the intricacies of contact dermatitis related to nail cosmetics, exploring the causes, symptoms, and preventative measures to safeguard your skin and your career.
The following table provides a summary of the key ingredients and their potential to cause allergic reactions.
- Mkvcinemas Kim The Ultimate Guide To Streaming Downloads And Beyond
- Dream With Satya Real Name The Journey Of A Rising Star In The Music Scene
| Ingredient | Common Use in Nail Products | Potential Allergenic Effects |
|---|---|---|
| (Meth)acrylates | Gel nail polish, acrylic nails, nail glues, base coats, top coats | Allergic contact dermatitis, skin irritation, blistering, itching, and nail abnormalities. Often the primary culprit. |
| Formaldehyde | Nail hardeners, nail polish | Allergic contact dermatitis, skin irritation, and in severe cases, respiratory problems. |
| Tosylamide/Formaldehyde Resin | Nail polish | Contact dermatitis and skin irritation. |
| Butyl Acetate | Nail polish solvent | Irritant contact dermatitis, and rarely, allergic reactions. |
| Colorants (Dyes and Pigments) | All types of nail products | Contact dermatitis, and nail surface discoloration (especially around the cuticle area). |
For further information, please refer to the American Academy of Dermatology: https://www.aad.org/public/diseases/eczema/types/contact-dermatitis/nail-products
Eyelid contact dermatitis due to artificial nails is rarely seen, especially outside of occupational settings, yet it does occur. More common is allergic contact dermatitis stemming from acrylic nail products, a trend that has been steadily increasing in recent years. This rise underscores the importance of understanding the risks associated with these cosmetic enhancements.
The diagnosis of allergic contact dermatitis is not always straightforward. It requires a careful assessment of the patient's history, including the products they use or come into contact with. A clear temporal relationship between nail cosmetic procedures and an eczematous outbreak on the hands, face, or other areas of the body can be a key indicator.
- Skymovies Hdin Your Ultimate Destination For Streaming Movies And Tv Shows
- Bolliflixcom The Ultimate Destination For Bollywood Enthusiasts
When a reaction occurs, physicians often recommend patients undergo patch testing. This process involves applying small amounts of various substances to the skin under controlled conditions to identify the specific allergen triggering the reaction. This is a crucial step in diagnosing and managing allergic contact dermatitis.
The differential diagnosis for dermatitis affecting the nail folds is broad and includes psoriasis, tinea manuum (a fungal infection), irritant contact dermatitis, and allergic contact dermatitis. Accurate diagnosis is critical for appropriate treatment.
The increasing occurrences of allergic contact dermatitis caused by acrylates in nail products are a significant concern. These acrylates can sensitize patients' immune systems, leading to reactions. Nail technicians and consumers alike are affected, highlighting the widespread nature of this issue.
One particular acrylate, Isobornyl acrylate (IBOA), a component found in coatings, sealants, glues, and adhesives, is gaining recognition for its role in causing allergic contact dermatitis. A case of ACD to IBOA in home nail glue has been reported, expanding the range of nail cosmetic allergens.
Many ingredients in nail products can sensitize the immune system. These include, but are not limited to, tosylamide, (meth)acrylates, and formaldehyde. Exposure to these chemicals can result in both allergic and irritant contact dermatitis reactions. The skin reacts either as irritant contact dermatitis or allergic contact dermatitis.
A contact allergy to acrylic artificial nails was first described in 1956. Since then, the popularity of gel nail polish (GNP) has exploded, creating new avenues for exposure to potential allergens. Research using databases like PubMed, Scopus, and Google Scholar has helped document the complications associated with GNP.
Ripping off gel polish can damage the natural nail, exposing it and increasing the risk of allergens penetrating the nail and possibly entering the bloodstream, initiating contact dermatitis.
Studies have been conducted to investigate the frequency and clinical features of ACD in nail cosmetics. These studies often take place in settings like university hospitals in locations like Amsterdam, Netherlands.
Other reported cases of dermatitis from nail enamels include allergies to solvents like butyl acetate and discoloration of the nail surface caused by colorants. Individuals with sensitivity to nail cosmetics can experience allergic and/or irritant contact dermatitis. Nail eczema and nail psoriasis, while sharing some similarities, are distinct conditions. While nail eczema can appear at any age, nail psoriasis typically affects older adults.
For nail salon workers, skin problems are common, including hand dermatitis, stomatitis, mechanical injuries, infections, and effects of ultraviolet radiation exposure. Hand dermatitis is frequently a result of irritant and allergic contact dermatitis, presenting in both acute "wet" and chronic "dry" forms.
Contact dermatitis of the nail unit can be either irritant or allergic, with ACD making up a significant portion of nail-related contact dermatitis cases. ACD of the nail apparatus often affects the proximal nail fold (PNF) and the hyponychium, which can lead to skin changes and nail plate abnormalities.
Allergic contact dermatitis (ACD) to cosmetics is very common, and it is a leading reason patients seek patch testing. The diagnosis should be initially suspected based on patient history and the distribution of the dermatitis. Low-allergenicity product recommendations should be implemented until patch testing is performed.
For nail professionals, contact dermatitis can be career-debilitating. With proper precautions in the salon, this can be avoided. One solution is to wear gloves.
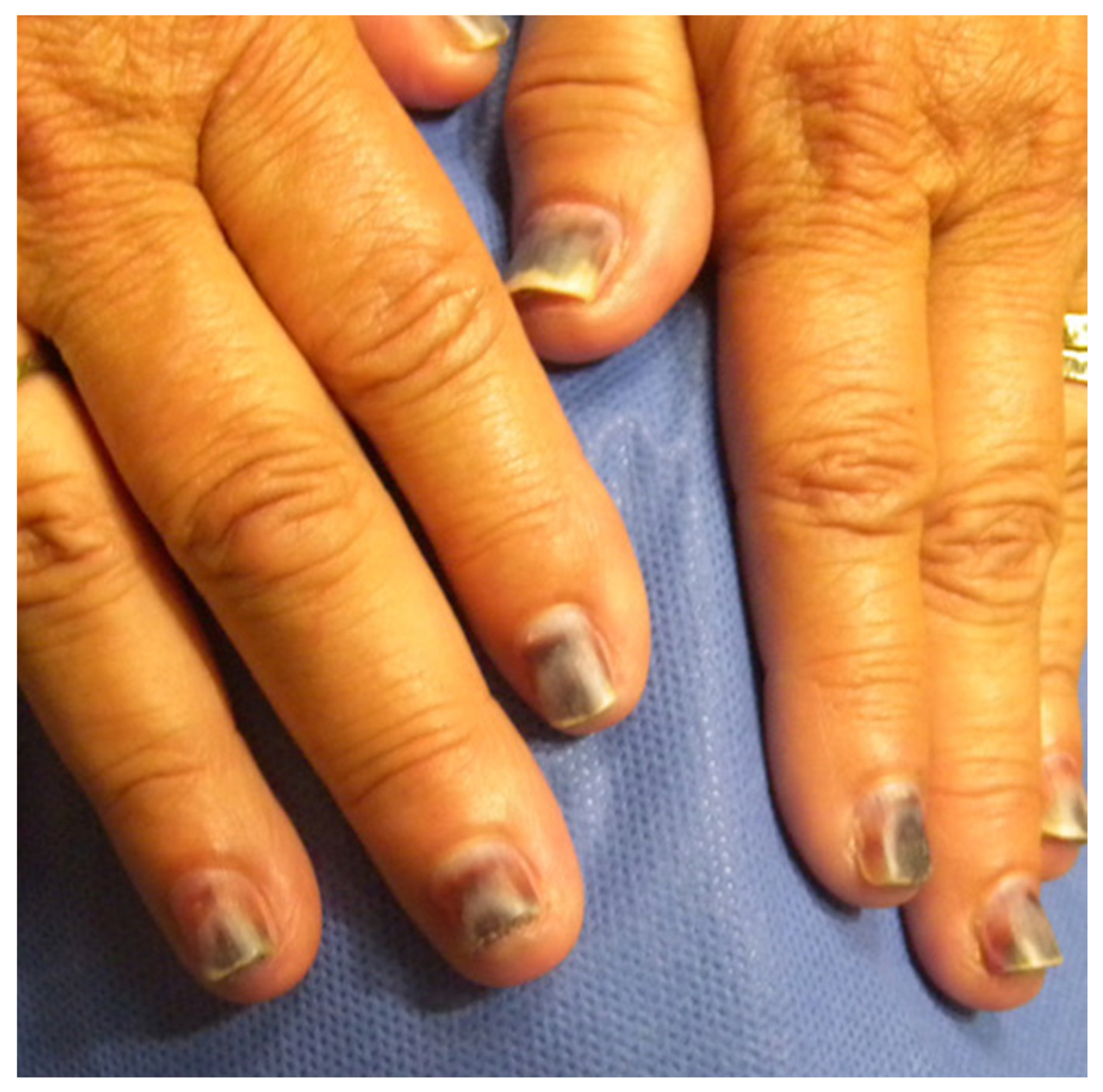
Materials, such as nail polish and nail enhancers, contain chemicals that can serve as contact sensitizers if they come into contact with periungual skin. Nail contact dermatitis can manifest as irritant contact dermatitis, with nail plate yellowing, nail dystrophy, and cuticle destruction, or as allergic contact dermatitis, with psoriasiform reactions on multiple fingernails.
Chemicals such as methyl acrylate are key contributors to allergies associated with gel nails. These acrylic compounds can induce skin irritation, often manifesting as contact dermatitis characterized by redness, itching, and blistering.
Contact dermatitis is an inflammatory skin condition that can be triggered by direct contact with irritants or allergens. The use of gel nails can result in either irritant contact dermatitis or allergic contact dermatitis.
The impact of nail products extends beyond simple cosmetic enhancements. When used incorrectly or without the proper precautions, these products can lead to allergic reactions, potentially causing significant discomfort. Therefore, a thorough understanding of the potential risks associated with these products is vital, especially for those who work with them professionally. Careful product selection, meticulous application techniques, and diligent adherence to safety protocols are crucial to minimize risks and ensure a positive experience for both the nail technician and the client.
- Dalia Dippolito Teeth The Shocking Story Behind The Bizarre Bite
- Sone385 Sub The Ultimate Guide To Unlocking Your Audio Experience